|
EXPERT REPORT
& WITNESS STATEMENT
DEATH OF BABY SUNAINA CHAUDHARI
b. 25/05/2000
d. 26/10/2000
24 March 2004
NEELU CHAUDHARI
BPharm MRPSGB Cert Ed
PHARMACIST
Reg No 075777
Ilford, Essex, UK
Tel/Fax Email
|
I have been a qualified pharmacist and a member of the Royal
Pharmaceutical Society of Great Britain
for over 20 years. My experience has been as Senior hospital pharmacist: advising
Consultants on the most appropriate and effective prescribing; as Pharmacist Manager: managing a retail pharmacy giving advice
to patients; and as Pharmacist Facilitator on behalf of health authorities, training other pharmacists to implement joint
projects with doctors. A copy of my membership certificate is attached, see p37.
I am compiling this expert report in respect of Sunaina Chaudhari,
who was born on 25/05/2000 and died 26/10/2000. I also act as an eye witness
to the detrimental effects on the child of the care she received prior to her death.
I have studied two medical files held for the child at King George Hospital
and Great Ormond Street Hospital respectively, including healthcare
records, CT scans, x-rays, pathology reports, toxicology reports, post-mortem reports and the transcript of the inquest.
I was unable to confirm the diagnosis of Trisomy 18 or Edwards
syndrome based on verbal diagnosis, in the absence of a Cytogenetics Laboratory report in the medical files.
Apart from a brief summary about the medical care provided,
for the purposes of this report, I intend to focus primarily on drug treatment in the period of two months prior to the death,
SUMMARY
This is a most horrific case of clinical and criminal negligence
involving a large number of medical professionals, causing the death of a 5 month old baby by drug overdoses and lethal poisoning
over a four week period. Those medical professionals defied all procedures, failed
to follow the advice of the Guy’s Poison’s Unit, and continued to with ranitidine drug overdoses for another 3
weeks in a way which they knew would cause the death of the child. Further, on
20/10/2000, whilst the child was suffocating from the drug
overdoses, they implemented an unlawful “DNR” or “Do Not Resuscitate” “withhold and withdraw”
and “palliative care” instruction against the medical opinion of two doctors, against the wishes of the parents
and without a court order. During the period of the “DNR”, these
professionals recommended, prescribed and administered lethal potassium chloride, without monitoring, without it being indicated
and in a manner which they knew would kill the child. Evidence from given at
the inquest by two doctors that the death was indeed as a result of the ranitidine overdoses and potassium chloride. I support a new inquest, a police investigation independent of the Coroner and a Public
Inquiry into this death. The Public Inquiry will investigate the current culture of multi-agency “social and medical
ambush”, a cause of high death rates, unaccountability and cover-up within the National Health Service.
A) Birth to disharge home (25/05/2000 – 01/08/2000)
Sunaina was born on 25/05/2000 at King George Hospital, Ilford,
Essex, full term +13days, by normal delivery, weighing 1.92kg, requiring ventilation pending surgery for a diaphragmatic hernia
repair (to reposition the stomach back into the abdomen which had slipped through the diaphragm into the chest area onto the
left lung, prior to birth). She was intubated and ventilated for 7 days prior
to a transfer to Great Ormond
Street Hospital for the repair
on 01/06/2000. A
spontaneous stomach perforation was found and repaired at the same time. She
was extubated, taken off mechanical ventilation to nasal CPAP oxygen on 06/06/2000
and returned to King George
Hospital on 08/06/2000.
Ranitidine IV and IV fluids were commenced on arrival. On 12/06/2000, Dr Shenoy stopped the ranitidine. On 13/06/2000, IV Dextrose saline was replaced
by oral hourly feeds. On 28/06/2000,
ranitidine was prescribed orally. [Ranitidine reduces acid production in the
stomach] On 12/07/2000,
she was on Frusemide and spironolactone.
The nasal CPAP was gradually weaned off onto low flow oxygen
from 13/06/2000 in preparation for discharge home on 01/08/2000. Discharge medication:
Frusemide, spironolactone, ranitidine. Weight 2.65kg.
B) AT HOME 01/08/2000 to 01/10/2000
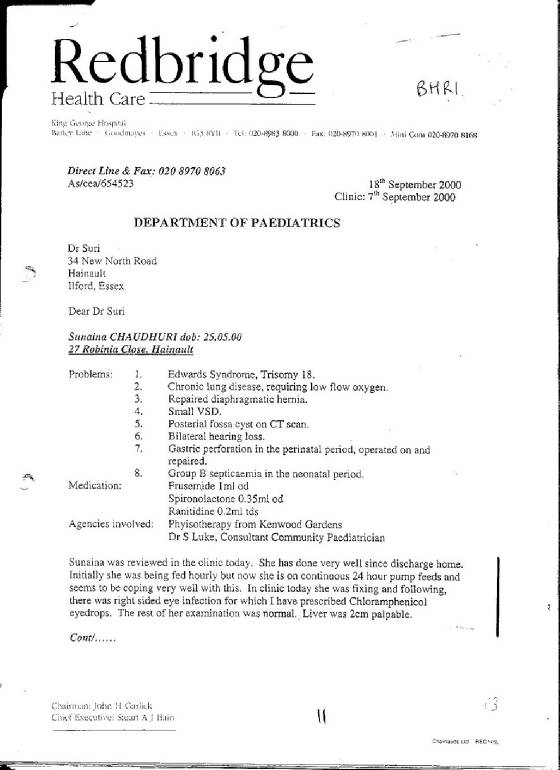
07/09/2000: See p11, 12.
Out-patient clinic examination by Consultant :Whilst living at home, Sunaina was examined in the out-patients clinic, King
George Hospital, by Paediatric
Consultant Dr Anand Shirsalkar on 07/09/2000, weight 3.55kg.
A letter was sent to GP Dr Suri and copied to Michelle Riceman, CNS Home Care Team, informing them
that Sunaina was currently on Frusemide 1ml daily, spironolactone 0.35ml daily and ranitidine 0.2mls three times daily, detailing
the plan:
“Dear Dr Suri, …Sunaina was reviewed in the clinic
today. She has done very well since discharge home. Initially she was being fed hourly but now she is on continuous 24 hour
pump feeds and seems to be coping very well with this. In clinic today she was fixing and following, there was right sided
eye infection for which I have prescribed Chloramphenicol eyedrops. The rest of her examination was normal. Liver was 2cm
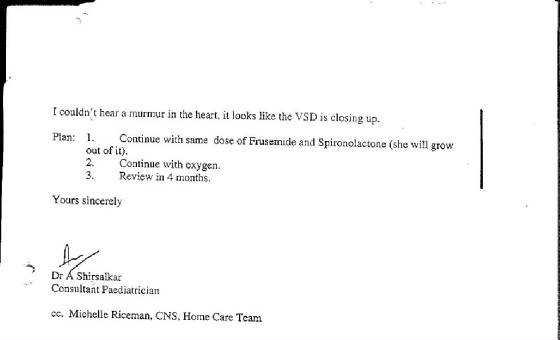
palpable; I couldn’t hear a murmur in the heart, it looks like the VSD is closing up. Plan: 1. Continue with same
dose of Frusemide and Spironolactone (she will grow out of it).2. Continue with oxygen. 3. Review in 4 months. Yours
sincerely Dr A Shirsalkar Consultant Paediatrician cc. Michelle Riceman, CNS, Home Care Team”
The plan was to continue with low flow oxygen at home, Frusemide
1ml (1mg) daily and spironolactone 0.35mls (1.75mg) daily. Ranitidine was not
part of this plan and was discontinued by Consultant Dr Shirsalkar. See page
11, page 12. A chest x-ray on 25/09/2000
was found normal.
26/09/2000: Adult dose prescribed by Dr Suri and dispensed By Tesco pharmacist
On 26/09/2000,
Sunaina’s father, Rajesh Kumar, collected a prescription for Sunaina from Dr Suri’s surgery. Dr Suri was negligent in prescribing ranitidine, when he had been notified in writing by Consultant
Dr Shirsalkar that it had been discontinued. He was negligent in prescribing
10mls twice daily, an adult dose to a 4 month old baby. He was also negligent
in prescribing 300mls, which is the usual amount prescribed for adults. The amount
is confirmed in the medical notes held by Dr Suri’s surgery. Dr Suri
was negligent in not reviewing the use of ranitidine in the child once discharged home and feeding by mouth.
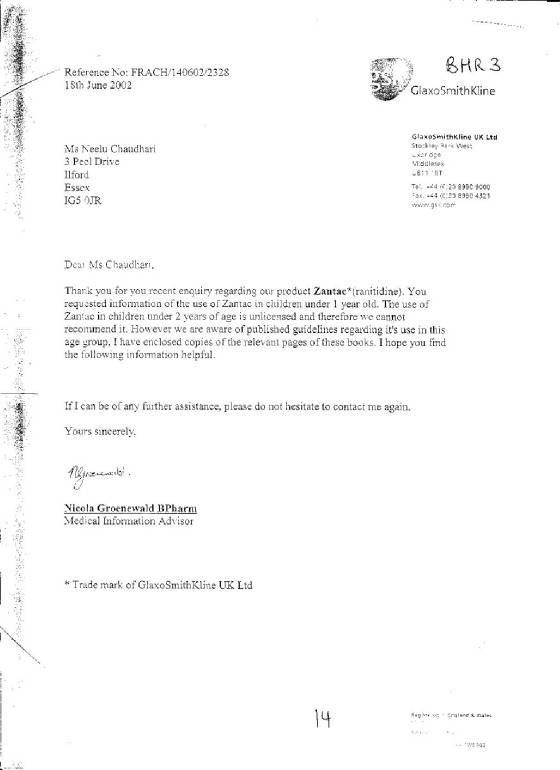
Ranitidine is unlicensed for use in children under 2 years
of age. See page 14. Manufacturers
for ranitidine (Zantac), Glaxo, list serious toxic effects on the heart and breathing and recommend it should be stopped immediately
with “sudden wheeziness or tightness in the chest”. They refer to
specialist paediatric guidelines for correct dosages when it is considered absolutely necessary. The dose in these cases is 1mg/kg three times daily, the child’s usual dose was 3mg three times
daily.
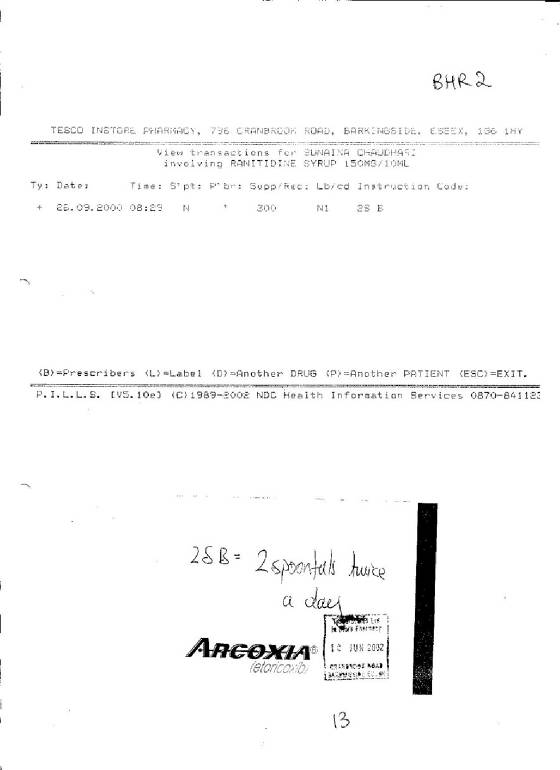
The adult dose of ranitidine was dispensed by Tesco Instore
Pharmacy, Barkingside at 08.29 hours on 26/09/2000.
“Ranitidine syrup 300ml, Two 5ml spoonfuls to be taken
Twice daily”.
Two 5ml spoonfuls, or 10mls is 150mg, an adult dose. This is fifty times the previous dose of 0.2mls prescribed for Sunaina, which had been stopped on 07/09/2000. A computer printout
on 10/06/2002 from the patient medication records for Sunaina
held by Tesco Pharmacy, Barkingside, Essex, confirm this. See page 13.
The pharmacist was negligent in dispensing an adult dose, 10mls
twice daily for a 4 month old baby. The pharmacist was negligent in dispensing
300ml for a 4 month old baby. The large volume in itself should have raised alarm
bells. Computers are programmed to give warnings to pharmacists when dispensing
medicines for children under 12 years of age. To avoid errors, the age has to
be entered and the overdose warning over-ridden before the label can be printed. The
time of the enquiry to Tesco was 10/06/2002, which is within
2 years of the date of the dispensing. The information as to who was logged into
the computer when the label was printed would have been in the computer records. I
have viewed correspondence with the Superintendant Pharmacist of Tesco, who failed to identify the pharmacist on duty. The name of the pharmacist “Raj Baxi” was the name put forward by Mr Ibbitt,
Pharmacy Inspector.
Sadhana Chaudhari queried the excessive volume for ranitidine
with Michelle Riceman and was advised on an amount to be administered. As a result
of the advice, the mother continued to administer an overdose of rantidine to her baby.
Michelle Riceman was negligent in advising on the administration whilst she had notification from Consultant Dr Shirsalkar
that the ranitidine had been discontinued. She was negligent in giving advice
she was not qualified to give and she should have referred the mother back to the hospital, GP or pharmacist.
26/09/2000: Assessment at King George Hospital
Later the same day, 26/09/2000, the child became unsettled, and was taken to King
George Hospital and examined.
“26/09/2000: Increased temperature, excessive crying…oxygen
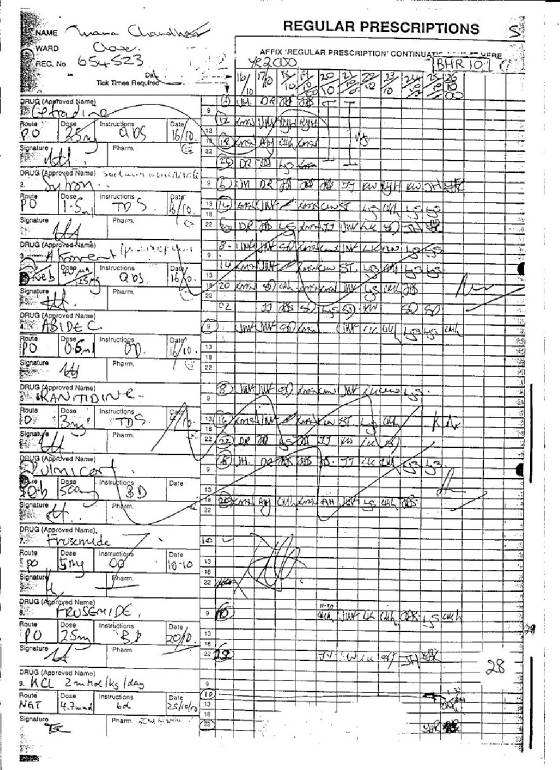
0.2-0.3 L…Meds – Ranitidine 30mg tds, frusemide 1ml od, spironolactone 0.35ml od, Abidec, Calpol PRN suppository
PR od.”
During this assessment, Ranitidine overdose was overlooked
as well as the fact that Consultant Dr Shirsalkar, had discontinued it on 07/09/2000. The child was prescribed “30mg ranitidine three times daily” and sent
home on the same thirty times overdose every 24 hours. See pages 15-16.
C) FIRST HOSPITAL ADMISSION LEADING TO DEATH
01/10/2000: First admission to King George Hospital for ranitidine
overdoses : On 01/10/2000, 01.00hrs, the child was taken to hospital for difficulty
in breathing and admitted to hospital. This was her first admission since her
discharge home on 01 August 2000. Dr Kathy Padoa examined Sunaina,
and was negligent in failing to note the overdoses being prescribed by King
George Hospital since 26/09/2000. Dr Kathy Padoa
failed to identify these overdoses as a cause of admission to hospital. See p16,
p17
Dr Padoa was negligent in failing to review the use of ranitidine
on admission when it was not indicated or recommended. She was also negligent
in failing to refer to the letter by Consultant Dr Shirsalkar in the medical file dated 07/09/2000 which recommended discontinuing it.
At 01.54hrs, pH 7.09, pCO2 10.2 kPa, pO2 5.1 kPa, HC03a 23.0mmol/L
tCO2 25.3mmol/L, BEvt -9.2mmol/L, O2sat 51.5%.
Dr Kathy Padoa was negligent in failing to commence nasal CPAP
(Continuous Positive Airways pressure) which was indicated for severe suffocation and critically low blood oxygen levels of
51.5% (normally 98%-100%). She was negligent to in allowing the child to continue
to suffocate at critical levels for over 12 hours.
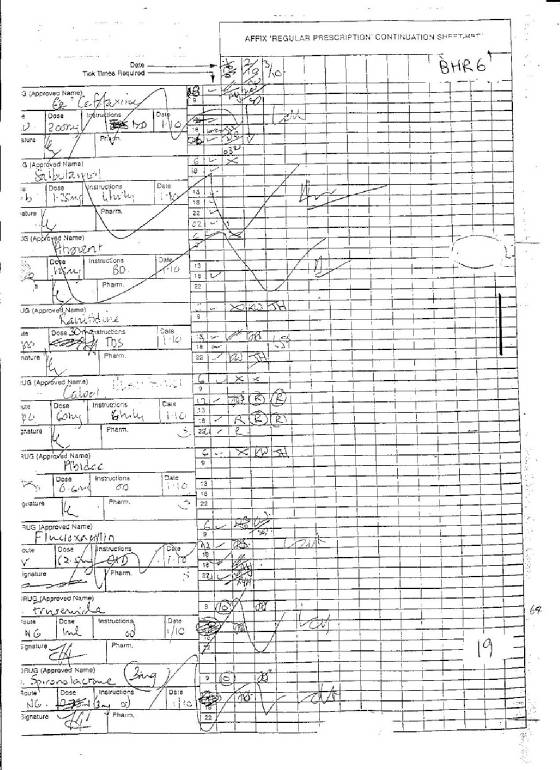
Dr Padoa was negligent in prescribing ranitidine 0.2ml three
times daily on the drug chart whilst Sunaina was having difficulty in breathing and increased oxygen requirements from ranitidine
overdoses. See page 19.
Later the same day, at 14.30hrs, the child was still suffering
severe effects of ranitidine overdoses, See page 17.
“Temp, resp distress, increased secretions…increased
oxygen requirement, normal 0.2L/min, now needing about 2L to keep sats above 91%...grunting, crying, irritable, oropharyngeal
secretions ++, pyrexial, HR 160-180/m, Chest: marked intercostal subcostal recession of chest ++ CVS: No heart murmur.”
On 01/10/2000, Dr Fran Harrowes altered the dose of ranitidine
from 0.2ml three times daily to 30 mg three times daily on the drug chart. As a result, the child received nine overdoses
of ranitidine of ten times overdose each, a total of ninety times overdose, whilst admitted to Clover Ward, King George Hospital
over a 4 day period to 04/10/2000. See page 19, entry no 4. and see page 20, entry no 3.
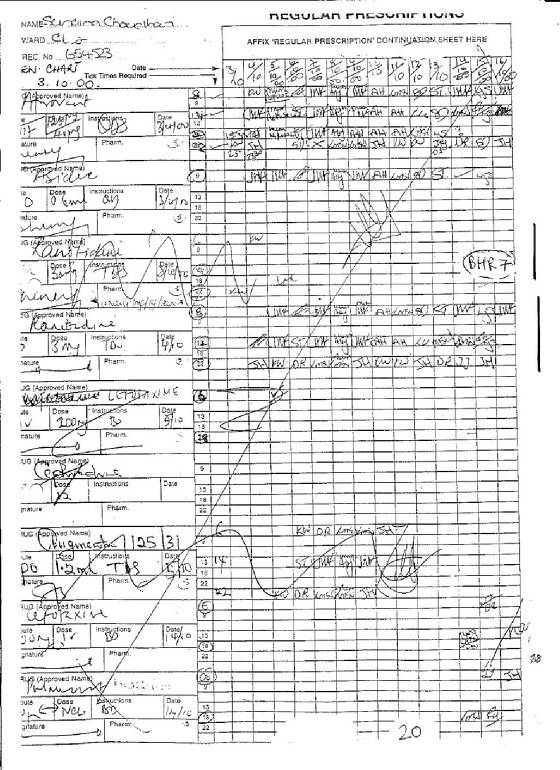
On 03rd
October 2000, Dr Shenoy was negligent in prescribing ranitidine 30mg three times daily on the new drug chart. Dr Shenoy was negligent in failing to review the use of ranitidine when it was not
indicated and failed to note that it had been discontinued by Consultant Dr Shirsalkar.
See page 20, entry no. 4. As a result two further doses of ranitidine
30mg were administered on 03/10/2000 and 04/10/2000.
The pharmacist, Rachel Soffe was the clinical pharmacist responsible
for Clover Ward and visited Clover ward daily where Sunaina was admitted. Rachel
Soffe failed in her professional duty to intervene the nine overdoses of ranitidine prescribed and administered to Sunaina
whilst admitted on Clover Ward. Rachel Soffe was negligent in failing to set
up recommended procedures to review medication on admission to hospital to identify drug overdoses as a cause of admission
and to halt a continuation of any drug overdoses administered prior to admission.
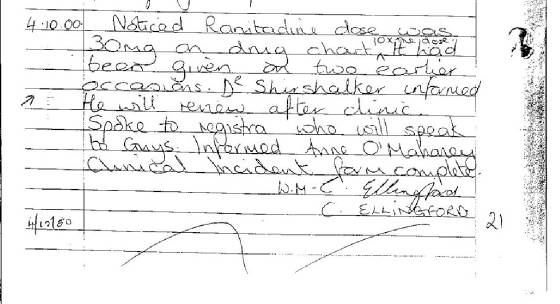
On 04/10/2000,
Dr V Gavel made an entry in the medical file in respect of his communication with Guys Poisons Unit following ranitidine overdoses
administered to the child whilst admitted to hospital.
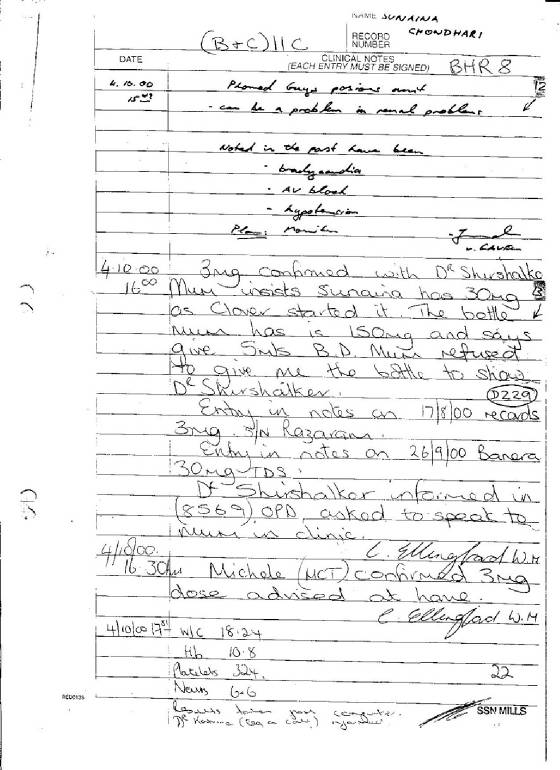
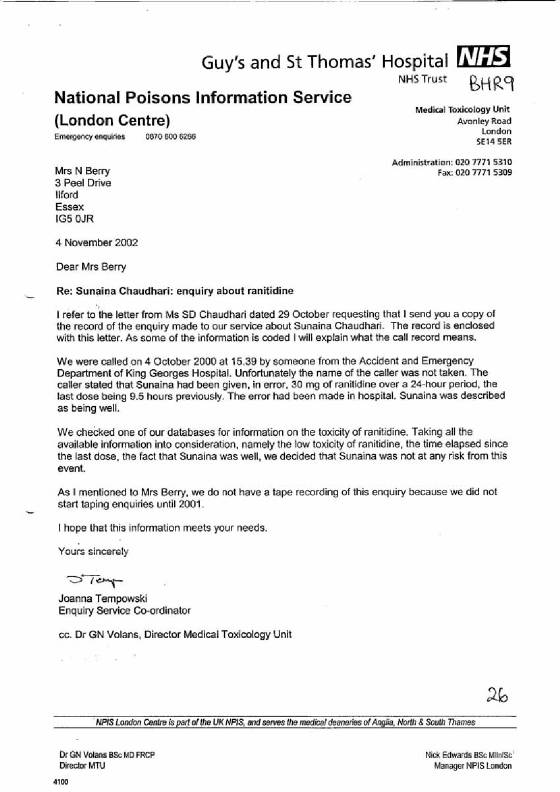
“Phoned Guys Poisons Unit, can be a problem in renal
problems, Noted in the past have been bradycardia, AV block, hypotension. Plan: Monitor …signed V Gavel”. See p22, top of page.
Dr Gavel was negligent in misinforming the Guys Poisons Unit
at 15.49hrs that 1) the child had come into accident and emergency, 2) she had received one single 30mg dose of ranitidine
in error, 3) the dose was given over 9 hours earlier, and 4) that the child was currently well. Dr Gavel was negligent in not informing the Guys Poisons Unit that 5) the child was prescribed the overdoses
during an in-patient stay over several days. He was negligent in giving them
6) the wrong information as to the time of the last doses, 30mg ranitidine at 06.00hrs and a dose of 3mg at 14.00 hrs on 04/10/2000.
In fact, Dr Gavel was negligent in not informing the Guys Poisons
Unit that 7) Sunaina had been administered some nine doses of ten times overdose each as prescribed by doctors followed by
8) an additional prescription on the drug chart for 3mg ranitidine three times daily since 14.00hrs, within two hours of his
communication with Guys Poisons Unit, to be continued indefinitely, 9) the first 3mg dose having been prescribed within the
last 2 hours. Dr Gavel then 10) failed to follow the advice by the Guys Poisons
Unit to monitor the child. See p21, p22, p23, p24, p25
The
label on the bottle dispensed by Tesco pharmacy, brought in by the mother was confirmed as having an adult dose of ranitidine, See and p21, p22, middle of page. No
clinical incident form was found completed in the medical file.
Rachel Soffe was negligent in not completing a clinical incident
form in respect of ranitidine drug overdoses administered during hospital admission even after the Guys Poisons Unit intervened
on 04/10/2000. She
was negligent in failing to advise on the discontinuation of ranitidine on advice from the Guys Poisons Unit. Rachel Soffe
was negligent that another dose of ranitidine was given at 22.00hrs on 04/10/2000, when the child’s oxygen level fell
further to 57.5% by 05.41hrs and 37.4% by 06.25hrs on 05/10/2000. Despite the critical level, another dose of ranitidine was administered at 08.00 hours
on 05/10/2000. See
page 20. An x-ray found the heart enlarged. See p25.
At 05.41hrs, pH 7.12, pCO2 7.7 kPa, pO2 5.3 kPa, HC03a 18.9mmol/L
tCO2 20.7mmol/L, BEvt -11.5mmol/L, O2sat 57.5%.
At 06.25hrs, pH 7.06, pCO2 15.9 kPa, pO2 4.2 kPa, HC03a 33.7mmol/L
tCO2 37.4mmol/L, BEvt -1.4mmol/L, O2sat 37.4%.
The pharmacist Rachel Soffe was further negligent in not intervening
whilst the child was continued with ranitidine at 3mg three times daily for another 3 week requiring nasal CPAP oxygen and
excessive suctioning for the resulting suffocation. See on page 28. The symptoms were worsening by 15/10/2000,
see page 29.
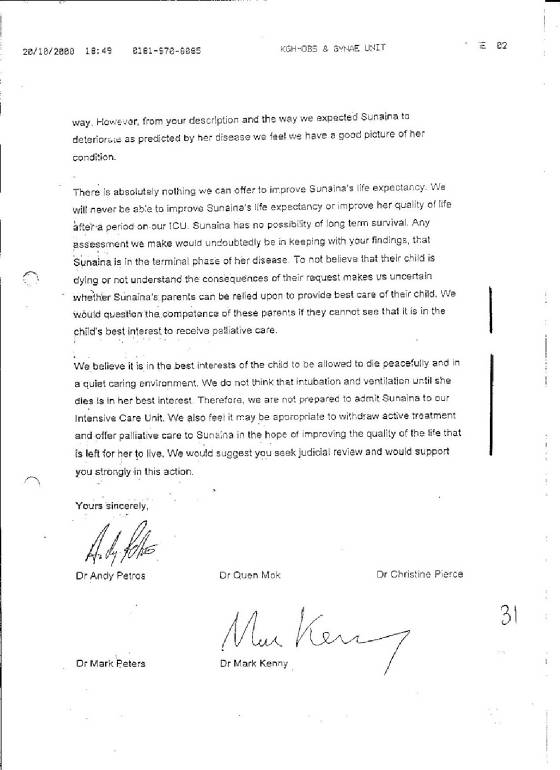
D) 20/10/2000: “DNR” Breach of Article 8 of “The Convention”
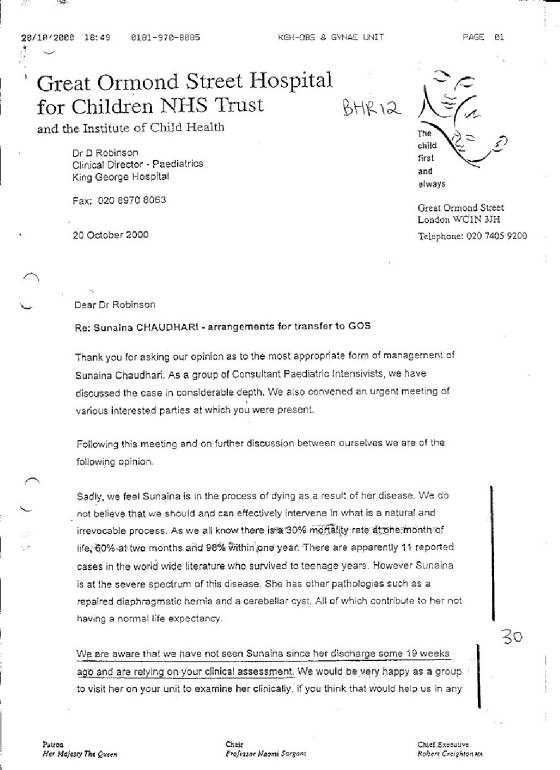
Fax “Second Opinion” from Great Ormond Street Hospital:
Consultants Dr Shirsalkar and Dr Robinson, King George Hospital, were negligent in advising 5 Consultants Drs Petros, Peters,
Kenny, Pierce and Mok, Great Ormond Street Hospital to issue a “Do Not Resuscitate”, “withhold and withdraw
active treatment” and “Palliative Care” order for Sunaina,
without an examination, without reviewing the medical file, without a Court Order, without discussions with parents and whilst
they knew she was suffering the toxic effects of ranitidine. See p30, p31
The
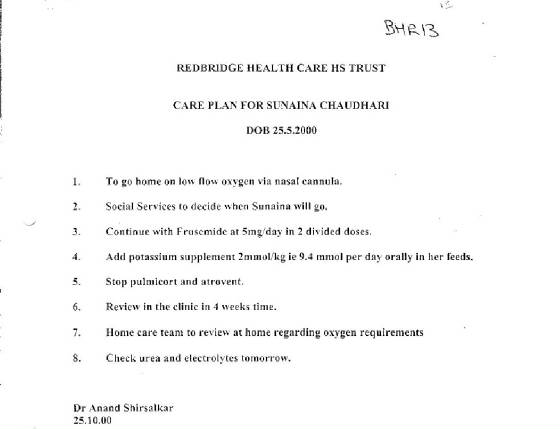
advice contradicted the medical examination and findings of two doctors at King George hospital on 19/10/2000, which found Sunaina improving and ready to wean off nasal CPAP. Dr Shirsalkar detailed a discharge plan dated 24/10/2000, to send Sunaina home. See page 32.
A visit made on 23/10/2000, to Clover Ward, King George Hospital,
by three Consultants from Great Ormond Street Hospital, Drs Petros, Kenny and Peters, signed “DNR” on Sunaina,
against the parents wishes, without a court order, whilst the ranitidine was being continued.
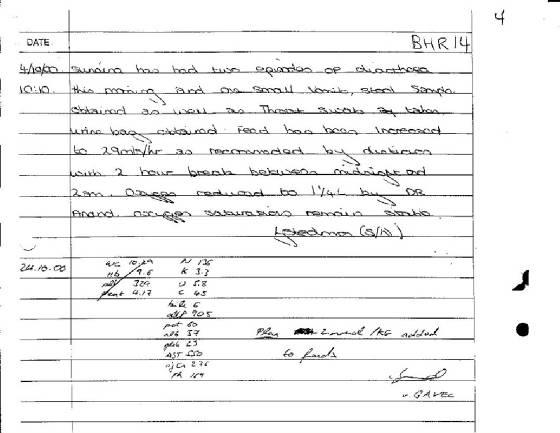
During the “DNR”, on 24/10/2000, Dr V Gavel prescribed lethal potassium chloride in the medical file, when it was
not indicated: See page 33.
N 136, K 3.3, U 5.8, C 4.5, bile 6, alkP 905, prot 60, alb
37, glob 23, AST 550, ajCa 276 ph 169
The child’s potassium level of 3.3mmol/L was due to frusemide
being prescribed and indicated the prescribing of spironolactone. Potassium Chloride
is a known lethal poison with a narrow therapeutic range. This means that it
can become lethal with small increases in levels and therefore requires blood monitoring before each dose and constant monitoring
of the heart during administration. It is also lethal when given at high speed,
therefore it must be administered very slowly. It must not be prescribed regularly
– only if required. It is normally administered in an acute setting, when
levels fall below 2.2mmol/L, not on a general ward. No such monitoring was done. Dr Gavel was negligent in prescribing “KCL” in the clinical notes on a
regular basis, long term, without specifying any monitoring or review. The “KCL”
is an abbreviation not normally used. His entry for “Plan KCL 2mmol/kg
added to feeds” has been tampered with by obliterating “KCL”.
Dr Thomas Rager was negligent in prescribing potassium chloride,
“KCL” on the drug chart on 25/10/2000 at a dose of 2mmol/kg/day, or 4.7mmol to be given regularly twice daily
via NGT, regularly, without any monitoring or review, when it was not indicated..
Dr Thomas Rager was negligent in administering Potassium chloride without monitoring or review. . Dr Thomas Rager was negligent in administering an additional
dose of potassium chloride prior to death - this dose appears on the drug chart at 22.00hrs on 26/10/2000, and was subsequently
obliterated. The time of death is documented as 11.10hrs on 26/10/2000, hence this dose must have been administered prior to death. See page 28.
Nurse Chris McMenamin was negligent in administering a dose
of potassium chloride at 13.30 hours on 25/10/2000 when it
was not prescribed by a doctor for that time. See page 28.
E) DEATH BY POTASSIUM CHLORIDE:
Dr Samarasekara was negligent in administering a dose of 4.7mmol
potassium chloride at 10.00hrs on 26/10/2000 without checking
blood potassium levels beforehand and without monitoring the effects on the heart. She
was negligent in failing to review the use potassium chloride. Dr Samarasekara
was negligent in recommending that Sunaina be commenced on antibiotics via a cannula, without monitoring. Dr Samarasekara failed to monitor Sunaina in the hour preceding the death.
Dr Samarasekara as paediatric consultant, in charge of Clover
Ward on the morning of 26/10/2000, was negligent in transferring Sunaina’s care to a more junior doctor, Dr Solebo,
SHO, who was on duty on another ward, SCBU, some 200m away, to enter Clover Ward so as to take over Sunaina’s care at
10.52hrs, seconds before her heart stopped. Dr Samarasekara was negligent in
supervising Dr Solebo to make repeated needle punctures in attempts at cannulation, without monitoring the heart and breathing. Dr Samarasekara failed to document in the medical file, details of monitoring and
drug administrations in the last hour of Sunaina’s life.
Pharmacist Rachel Soffe was negligent in failing to advise
doctors that potassium chloride was inappropriate for the child, that spironolactone was appropriate, that that regular doses
of potassium chloride without monitoring could be lethal. Rachel Soffe was negligent
in supplying a bottle of potassium chloride from pharmacy to the doctors without giving advice on its correct use, review
and monitoring, knowing that its use would be lethal.
Lack of chromosome evidence of Trisomy 18
I contacted the Great
Ormond Street Hospital
for a copy of a Cytogenetics report with photographic evidence of the chromosome tests carried out on 6 cells by Louise Wilson
. I was advised on 16/03/2004,
by genetics nurse specialist Bernadette Farren, responsible for Sunaina, that she herself had never seen it. In its absence there is no evidence to suggest that Sunaina had Trisomy 18 except verbal evidence. Throughout the medical file, all internal organs were found to be working normally,
apart from a “very small VSD” of the heart which was found clinically closed on 07/09/200 and the small left lung
size at birth, which was found to be the same size as the right lung in an x-ray mid September 2000.
Lack of evidence of Edwards Syndrome
“Edwards Syndrome” is a condition, a hypothetical
collection of possible symptoms, which may or may not be present in a person confirmed as having Trisomy 18. In the absence of a confirmed diagnosis of Trisomy 18, the term is a theoretical invention in much the
same way as Professor Sir Roy Meadows’ Munchausen Syndrome by Proxy. “Edwards
Syndrome” is neither an illness, nor a disease, nor a possible cause of death. In the absence of a diagnosis of Trisomy
18 in Sunaina, any reference that she had Edwards Syndrome is therefore not justified.
Massive evidence that Sunaina was a normal
baby
All predictions by various doctors were proved wrong when Sunaina
did not die inside her mother’s womb, did not die during birth, immediately after birth or during the diaphragmatic
hernia operation. In fact she amazed doctors with the speed of her recovery,
returning to King George
Hospital in a week after the diaphragmatic hernia operation. Many doctors commented on how they thought Sunaina looked and behaved like a normal baby. This is confirmed by the growth chart for Sunaina which indicates she was growing at a slightly higher
rate than normal. Sunaina was smiling, cooing fixing and following, and sitting
up unaided at four and a half months.
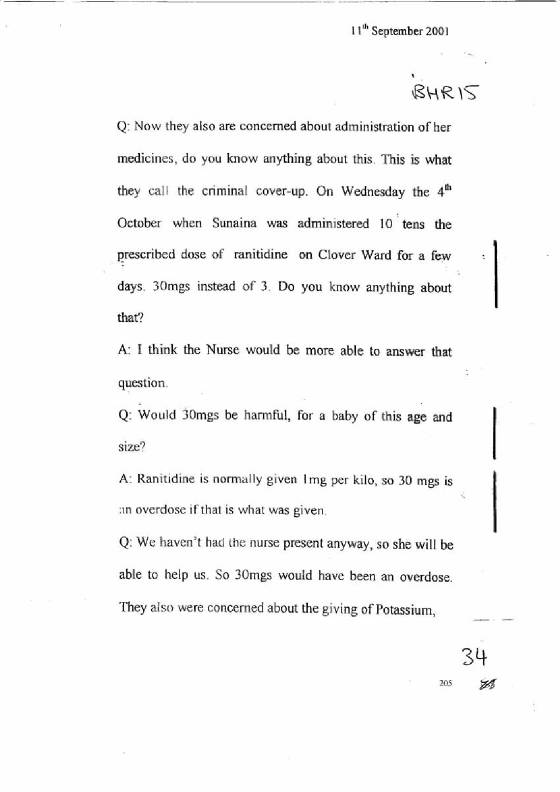
Inquest Evidence on ranitidine overdoses
and lethal potassium chloride
Consultant Dr Shirsalkar gave evidence at the inquest that
Sunaina was given several overdoses of ranitidine in error. He further gave evidence
that he would not have prescribed potassium chloride as it is lethal and could stop the heart.
See p34, p35, p36.
Dr Solebo gave evidence
at the inquest that the child’s heart did stop suddenly.
Evidence of tampering of Medical File &
Forgery
Having inspected the original medical file held at King George Hospital,
there was much evidence that pages had been ripped out, shuffled, removed, replaced inserted and re-inserted. Reinforcers had been placed on both sides of punched holes of pages which had been ripped out and reinserted
on a second viewing. The last drug chart which had details of potassium chloride,
was found with a bundle of documents inserted inside it. There were many blank
pages which had been crossed out giving the impression that they had been written and inserted retrospectively. Doctors were not consistent in recording times for the clinical notes entries. Discontinuation of drug treatment and alterations were not always dated or signed.
F) CONCLUSION:
NOTE: The ECHR ruled on 09/03/2004, in Glass V UK,
Application no. 61827/00, that “DNR”
implemention without parents knowledge or consent is a breach of Article 8 of the Convention for the Protection of Human Rights
and Fundamental Freedoms (“the Convention”).
The above report finds the above named were negligent clinically
and criminally in their medical, clinical pharmacy and nursing care provided to baby Sunaina Chaudhari leading to her death
by ranitidine overdoses and lethal potassium chloride poisoning.
Signed:
……………………………………………
Neelu Chaudhari
BPharm MRPSGB Cert Ed.,
Ilford, Essex |